
Children at Risk
Gaps in State Lead Screening Policies

Executive Summary
There is no safe level of lead in a child’s blood. Very young children are particularly vulnerable, even at low levels. While lead has been banned from household paint and gasoline for some time, there are numerous sources of exposure, including paint in older housing, water service lines and plumbing, and several continuing commercial uses. Primary prevention strategies that eliminate these sources are still the best way to prevent exposure to lead. Safer Chemicals, Healthy Families advocates for strong primary prevention policies. Nevertheless, regular blood lead testing is critical for identifying very young children with elevated levels early enough that intervention can prevent or mitigate long-term developmental damage.
This report takes a detailed look at each state’s blood lead testing policies. After comparing state programs by the percentage of children tested in recent years, the report discusses why some policies have been ineffective, and focuses on key reasons for higher testing rates reported in other states. The report concludes with a critique of targeted testing strategies and calls on states to move to universal screening to better protect their children.
State Lead Testing Policies
Key Findings
- The patchwork of blood lead screening policies is inadequate and likely misses a significant number of children with elevated lead levels during the critical window when intervention could prevent long-term damage.
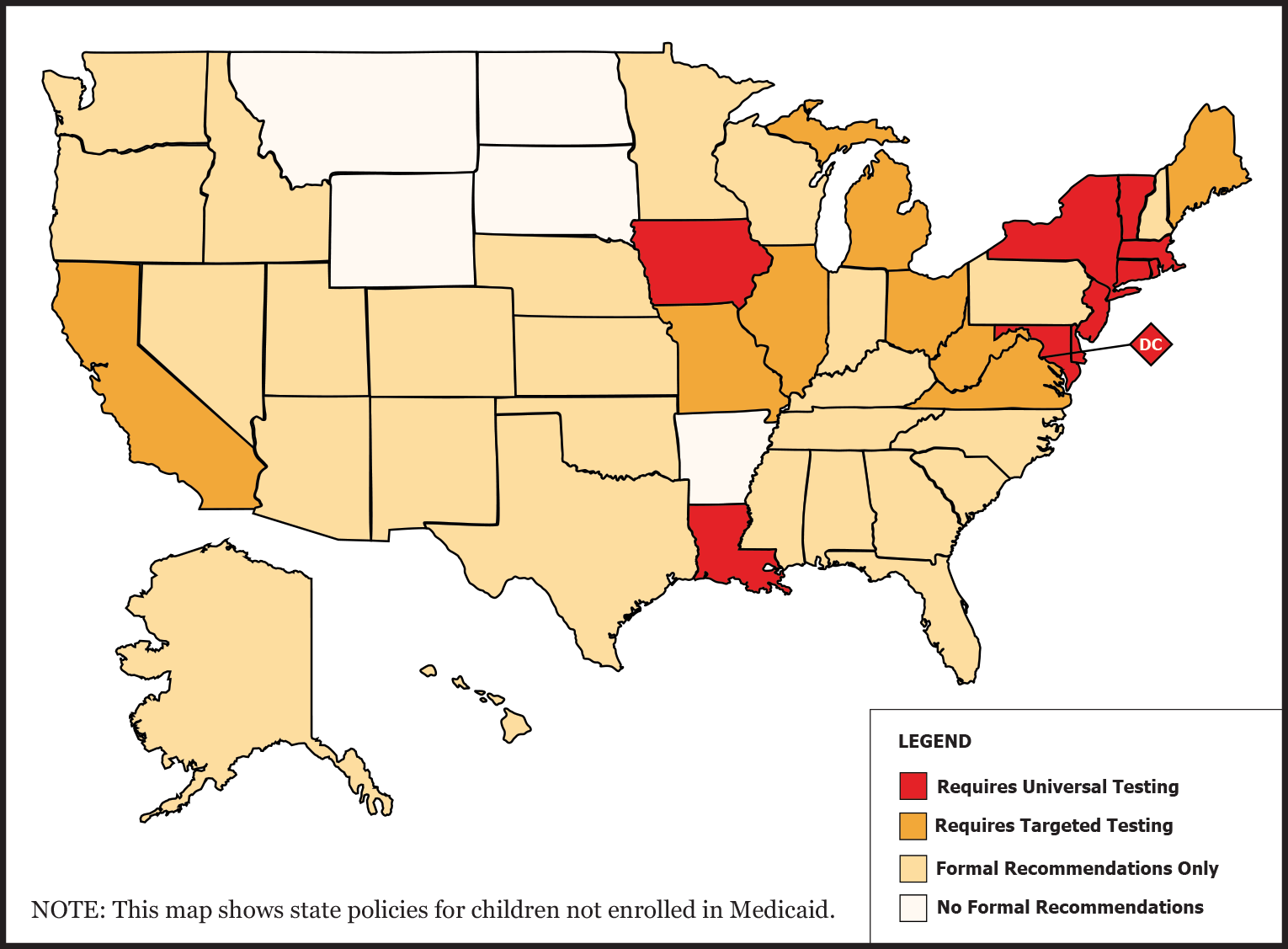
- State lead screening policies (non-Medicaid) span a range of possibilities:
- 10 states plus D.C. require universal testing, generally for all children at ages 1 and 2;
- 8 states require targeted testing;
- 27 states only provide recommendations; and
- 5 states have no requirements or recommendations on their websites.
- 45 states plus the District of Columbia say clearly that they follow the federal requirement on testing for children enrolled in Medicaid.
- While a few universal testing states come close, no state is 100% compliant with federal Medicaid requirements or general state policies that require testing children at the critically important ages of 1 and 2.
- Several states have taken action to maximize testing rates. They require universal screening, educate providers and parents about the mandate, and make blood lead tests easier to obtain. Some require proof of a lead test for school enrollment.
- Universal testing is more useful and cost-effective than targeted testing. Targeted testing strategies are unlikely to successfully identify all of the children at risk for lead exposure.
Recommendations for States
- Adopt universal testing to discover the full extent of blood lead levels above the federal reference level of 5 micrograms per deciliter.
- Implement strategic education campaigns for health care providers and parents.
- Make the testing accessible and affordable.
- Require universal reporting of test results.
- Publish data on tests done at both 12 and 24 months.
Read the Full Report
- I.Methodology
- II.Introduction
- III.Federal Testing Policies and Funding
- IV.State Lead Screening Policies and Reporting Requirements
- V.State Policies for Testing Medicaid-enrolled Children
- VI.Best Practices: Highlights From Successful Programs
- VII.Universal versus Targeted Screening
- VIII.Conclusion and Recommendations
- IX.Endnotes
- X.Table 1.A
- XI.Table 1.B
- XII.Table 1.C
- XIII.Table 1.D
- XIV.Table 2